

Interact Sensitively with Employees Addicted to Opioids
Opioid addiction is running rampant across the U.S. According to the National Institute of Drug Abuse, 8-12 percent of patients prescribed opioids develop an opioid use disorder. Read this blog post to learn more.
Employees who abuse opioids often are given a second chance by their employers. But well-meaning employers could wind up being sued for discriminating against those workers in violation of the Americans with Disabilities Act (ADA) if they don't handle the situation very carefully.
Opioid addiction has been rampant in the U.S. for some time. More than three out of five drug overdose deaths last year involved an opioid, and overdoses rose 70 percent in the 12 months ending September 2017, according to the Centers for Disease Control and Prevention.
So what can HR professionals do about it? If a worker admits to the problem, the path is fairly clear. But if the employer merely suspects that an employee is addicted to prescription pain relievers but has no real proof, the employee should be treated like any other employee who is having attendance or performance issues, said Kathryn Russo, an attorney with Jackson Lewis in Melville, N.Y.
An employer should never accuse someone of having an addiction, because if the employer is wrong, the accusation could lead to an ADA claim, Russo cautioned. Although current drug use isn't considered an ADA disability, a history of drug addiction is. Moreover, someone using prescription drugs might have an underlying condition covered by the ADA.
If an employee admits to opioid abuse, or the problem is discovered through drug testing, the employer should discuss it with the employee to determine if he or she needs a reasonable accommodation, such as leave to obtain treatment, Russo said. The illegal use of drugs need not be tolerated at work, she added.
Reasonably accommodate the employee so long as there's no direct threat to the health and safety of himself or herself, or others, recommended Nancy Delogu, an attorney with Littler in Washington, D.C.
Drug Testing
The Equal Employment Opportunity Commission has opined that employers may ask about an employee's use of prescribed medicine or conduct a drug test to determine such use only if the employer has reasonable suspicion that its use will interfere with the employee's ability to perform the job's essential functions or will pose a direct threat.
Many employers are expanding their drug-testing panels to include semisynthetic opioids such as hydrocodone, hydromorphone, oxycodone and oxymorphone, in addition to traditional opioids such as heroin, codeine and morphine, Russo said. This is lawful in most states as long as the employer does not take adverse employment actions when drugs are used legally, she noted, which is why an employer should use a medical review officer in the drug-testing process. If the medical review officer concludes that the positive test result is the result of lawful drug use, the result is reported to the employer as negative.
Sometimes an employer will say it has reasonable suspicion that the employee came to work impaired by drug use and is considering a mandatory drug test. At that point, some employees will say the drug test would be positive and the test consequently is not necessary.
Discussions with Employees
If there are performance problems and the employee has admitted to opioid addiction, some employers tell employees that they can remain employed so long as they go through inpatient treatment. Delogu discourages that approach. Employers aren't workers' doctors, so they shouldn't be deciding whether someone needs a treatment program, she explained.
But if someone voluntarily seeks to enter an addiction-recovery program, that person may have legal protections under state law, said Wendy Lane, an attorney with Greenberg Glusker in Los Angeles. For example, California has a law requiring employers with 25 or more employees to reasonably accommodate alcohol and drug rehabilitation.
Delogu recommended that employers that believe there is a problem with substance abuse ask if the addicted employee needs assistance from the employee assistance program.
An employer can require that an employee who has violated a policy be evaluated by a substance abuse professional and complete treatment prescribed for them, without dictating what that treatment will be, she said. The employer may choose to forgo disciplinary action if an employee agrees to these terms and signs an agreement to this effect. The employer then would not have to be informed about the person's decided course of treatment, whether inpatient, outpatient or no treatment at all, she said. The employee typically will be subjected to follow-up drug testing to make sure he or she hasn't resumed the use of illegal drugs.
Many employers are willing to give employees with performance problems resulting from opioid addiction a second chance, she noted.
SOURCE: Smith, A. (1 November 2018) "Interact Sensitively with Employees Addicted to Opioids" (Web Blog Post). Retrieved from https://www.shrm.org/ResourcesAndTools/legal-and-compliance/employment-law/Pages/employees-addicted-to-opioids.aspx

What employers can do to combat risks of workplace opioid abuse
How can employers combat the risks associated with workplace opioid abuse? With an increase in opioid use, employers are now tasked with the challenge of addressing opioid misuse in the workplace. Continue reading to learn more.
The opioid epidemic presents a unique challenge for employers. While opioids can be beneficial for employees suffering from pain, they also pose grave risks and dangers for companies as even appropriate use of the drugs can cause impairment and lead to accidents.
For example, if an employee had an accident and suffers an injury, you may see the physical signs of the injury. However, it’s not as obvious if the employee was prescribed opioids for the pain associated with that injury. If the employee doesn’t disclose the prescription, they could resume their everyday duties, like operating machinery, when they should be restricted while using the drug.
Due to the increasing prevalence of opioid use, employers are likely now challenged with addressing misuse in the workplace. Often, companies may not know the best approach to supporting employees dealing with an opioid addiction. When speaking with employers, it’s important to stress the need for organizations to be well-versed in opioid misuse and ways to proactively identify and address it.
Employers can work to combat opioid use in their organization by providing accommodations and updating their policies, procedures and employee communications. Here are a few ways they can get started.
Short-term accommodations
If an employee is taking prescribed opioids for an injury and has specific limitations or restrictions, an employer can work with a disability carrier to determine potential short-term accommodations that can be made to meet the employee’s needs. Short-term accommodations can help keep an employee comfortable and productive at work during his or her recovery.
Policies and procedures
If an employer hasn’t done so already, it should consider putting a comprehensive drug policy in place to help it address issues that may arise if an employee misuses prescription drugs. The policy should include a description of available assistance options for employees who are struggling with substance abuse and clearly state consequences for employees who violate the policy, empowering supervisors to take appropriate action in response to employee issues.
Destigmatizing use
It’s easier to help someone if they come forward, but right now, stigma surrounding opioids can cause employees to keep their prescription use to themselves. Encouraging open lines of communication can help companies destigmatize prescription drug use so their employees feel comfortable disclosing the medications they’re taking that could limit them at work.
Fostering transparency, combined with short-term accommodations and clear policies, can help employees feel more comfortable coming forward with their condition. Remind employers that their disability carrier can be a great resource to help with education, recommend proactive ways to address misuse at their organization and create accommodation plans for employees in need. With these steps, employers can help support their employees and, ultimately, make the workplace a safer place for all.
SOURCE: Jolivet, D (16 October 2018) "What employers can do to combat risks of workplace opioid abuse" (Web Blog Post). Retrieved from https://www.benefitnews.com/opinion/what-employers-can-do-to-combat-workplace-opioid-abuse-risk

Senate passes bill to combat opioid epidemic
Recently, the Senate passed a bill to help battle the opioid crisis. This bill is designed to battle opioid and other prescription drug misuse within the United States. Read this blog post to learn more.
Both parties got behind a bill designed to fight the misuse of opioids and other addictive medications, with a sole Republican voting against it as it passed in the Senate.
See also: Employers take steps to address opioid crisis
As reported by the Associated Press, Utah Republican Mike Lee was the sole dissenting voice as the bill was passed 99-1.
According to the reports, the legislation’s reach is broad, with provisions for deeper scrutiny of arriving international mail that could contain illegal drugs; money for the National Institutes of Health research on nonaddictive painkillers; paving the way for pharmaceutical companies to conduct research on alternatives; approval for the Food and Drug Administration to require drug manufacturers to provide opioids and similar drugs in smaller quantities and packages; and provides federal grants for treatment centers, emergency worker training and prevention research.
See also: The days of employers ignoring the opioid crisis are over
It also would push physicians to discuss pain management alternatives with Medicare patients, something that could have an effect on Department of Health and Human Services data indicating that a third of Medicare Part D prescription plan users in 2017 were prescribed opioids.
“I recognize these provisions are just a start, but we are losing 116 lives every day. And we need to save as many as we can—as soon as we can,” Sen. Gary Peters (D., Mich.) told the Senate.
Funding for the provisions of the measure will have to come from separate spending bills, and for the bill to become law, it will have to be reconciled with legislation that passed the House back in June. Despite the high level of tension between Democrats and Republicans at present, according to the Wall Street Journal, “Senate aides are optimistic the measures can be reconciled and passed by the end of the year.” Still, opioid use is definitely a bipartisan issue, hitting red and blue states alike, with preliminary data from the Centers for Disease Control and Prevention indicating that in 2017 U.S. overdose deaths from all drugs set a record and ballooned to more than 72,000.
SOURCE: Satter, M. (18 September 2018) "Senate passes bill to combat opioid epidemic" (Web Blog Post). Retrieved from https://www.benefitspro.com/2018/09/18/senate-passes-bill-to-combat-opioid-epidemic/

The days of employers ignoring the opioid crisis are over
What do employers need to know to help their employees and help reduce the risk of the opioid crisis? The opioid crisis is affecting companies' productivity, medical claims, work injuries and their bottom line. Read this blog post to learn more.
Productivity, medical claims, work injuries, and the company’s bottom line — what do these things all have in common? They are all being drastically affected by the effects of substance abuse. The opioid crisis that is running rampant across the United States is having an impact on employees at every level.
As an employer, what do you need to know to support your employees and reduce the risk of this national crisis?
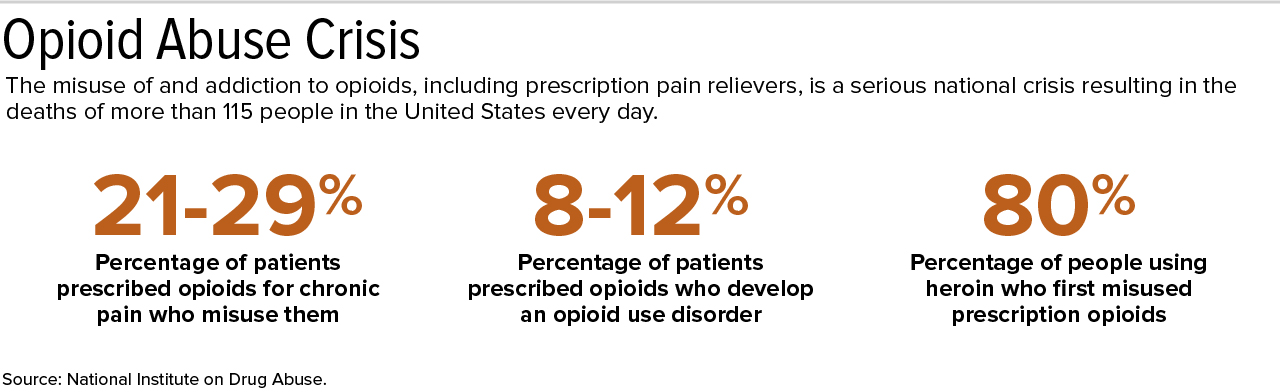
First, you need to educate yourself on the facts. According to the National Institute on Drug Abuse, every day, more than 115 people in the U.S. die after overdosing on opioids. It is not just the deadly heroin/fentanyl combination that we have been hearing about in the news, sources of opioid addiction include prescription pain relievers such as hydrocodone, oxycodone, oxymorphone, morphine, codeine, and other prescribed substances.
See also: Taking A Page From Pharma’s Playbook To Fight The Opioid Crisis
The Center for Disease Control and Prevention estimates prescription opioid misuse in the U.S. cost $78.5 billion per year; affecting medical spend, productivity, and law enforcement supervision.
Substance abuse does not discriminate on any demographic, however if your business is construction, entertainment, recreation, or food service, the National Safety Council found your employees are twice as likelyas the national average to have substance abuse disorders.

Secondly, you need to take action. The most important thing an employer can do is to have a proactive plan in place to help your employees live a healthy lifestyle. It is easy to get in the habit of saying “that does not happen here,” but the reality is substance abuse can — and does — happen anywhere.
Solving the opioid crisis won’t happen overnight, but here are some steps to take to build a better relationship with your employees and quite possibly help someone overcome a substance abuse problem.
Train your staff. Explain what resources are available to help them help your employees. If you have an employee assistance program in place, leverage it, and have the information easily available so any employee can access the information at any time. This will help lower the fear barrier for employees who are not ready to ask someone they know for help. If you do not have the right resources in place today there are many programs available, and it is important that you adopt one that will fit your culture and help employees be high performers.
See also: Employers take steps to address opioid crisis
Show employees you care. Look for signs and symptoms that an employee might have a problem with substance abuse. Make sure supervisors, managers, and team leaders are aware of these signs and what actions they should take. Have an open door policy, and make sure your employees feel they can ask for assistance when they need it. It is important to know how to handle sensitive, often painful, discussions in a professional and action-oriented manner. It is essential that you have the right steps in place to ensure leadership is aligned with the organization’s strategy on how best to help your at-risk population.
Be transparent. Have clear policies in place that promote a drug-free workplace. Consider expanding your drug testing panel to include opioids.
Share the savings. Consider sharing the dollars a successful well-being program will save your organization’s bottom line through lower prescription drug costs and less lost productivity due to illness and time away from work.
See also: A look at how the opioid crisis has affected people with employer coverage
If your organization is struggling with how to successfully address the challenges of substance abuse and opioid addiction, seek out employee benefit consultants to help you develop a strategy for success. Like anyone with an addiction, there is no shame in asking for help.
SOURCE: Panning, C (7 September 2018) "The days of employers ignoring the opioid crisis are over" (Web Blog Post). Retrieved from https://www.benefitnews.com/opinion/employers-cannot-ignoring-the-opioid-crisis?feed=00000152-a2fb-d118-ab57-b3ff6e310000

Employers take steps to address opioid crisis
By addressing opioid misuse, employers could in turn have more productive workers and lower healthcare costs. Continue reading to learn more.
President Donald Trump declared the nation's opioid crisis a "public health emergency" last month, underscoring employer concerns about this growing epidemic.
The opioid crisis cost the U.S. economy $95 billion in 2016, and preliminary data for 2017 predict the cost will increase, according to a new analysis from Altarum, a health care research and consulting firm. Addressing opioid misuse could lead to more productive workers and lower health care costs.
U.S. employers are increasingly seeking ways to reduce the abuse of prescription opioids, according to new findings from the Washington, D.C.-based National Business Group on Health (NBGH), which represents large employers.
NBGH's Large Employers' 2018 Health Care Strategy and Plan Design Survey found that the vast majority of big employers (80 percent) are concerned about abuse of prescription opioids, with 53 percent stating that they are very concerned. Thirty percent have restrictions for prescription opioids, and 21 percent have programs to manage prescription opioid use.
The survey was conducted between May 22 and June 26, and reflects the strategies and plan offerings of 148 U.S. employers, two-thirds of which belong to the Fortune 500 or the Fortune Global 500.
"The opioid crisis is a growing concern among large employers, and with good reason," said Brian Marcotte, NBGH president and CEO. "The misuse and abuse of opioids could negatively impact employee productivity, workplace costs, the availability of labor, absenteeism and disability costs, workers' compensation claims, as well as overall medical expenses."
Given the widespread nature and expanding scope of the opioid crisis, some employers are working directly with their health plans and pharmacy benefit managers (PBMs) to address the issue, the survey showed. Those that are working to manage opioid use most often use the following strategies:
- Limiting the quantity of pills on initial prescriptions for opioids.
- Limiting coverage of opioids to a network of pharmacies and/or providers.
- Expanding coverage of alternatives for pain management, such as physical therapy.
- Providing training in the workplace to increase awareness and recognition of signs of opioid abuse.
- Working with their health plans to encourage physicians to communicate about the dangers of opioids and to consider alternatives for pain management.
Apart from these measures, employers are:
- Increasing communications and training for managers and employees to raise awareness of the issue.
- Identifying people who may be at risk for addiction who could benefit from help.
- Encouraging employees to take advantage of an employee assistance program, the health plan and other resources for help and treatment.
Different Pain Management Approaches
Janet Poppe, senior director for payer and employer relations at Pacira Pharmaceuticals, based in Parsippany-Troy Hills, N.J., advises using a multitherapy pain management strategy to minimize opioid use—especially following surgery, which she called "the gateway to the opioid epidemic."
"Opioid monotherapy is the current standard of care for postsurgical pain management," Poppe said on Nov. 14 at the National Alliance of Healthcare Purchaser Coalitions' 2017 annual conference, held in Arlington, Va. She cited research showing that:
- 98.6 percent of inpatient surgery patients receive opioids to manage postsurgical pain.
- 92 percent of postsurgical patients who receive opioids for acute pain report adverse side effects such as urinary retention or respiratory depression, the treatment of which can be costly.
In another study, more than 10 percent of patients who were prescribed an opioid within seven days of surgery were identified as long-term opioid users one year after surgery. Other research shows that 1 in 15 patients who receive an opioid post-surgery become chronic users.
Local anesthetics, anti-inflammatory drugs and nonopioids such as sodium-channel blockers are among the options available to address pain without the addictive and debilitating effects of opioids, Poppe said. "Using two or more nonopioid pain relievers that act on the body in different ways can produce a better result, at a lower cost, than using opioids."
"There is a need to generate widespread public awareness of the role that postsurgical opioids play in the larger public health crisis in the U.S.," Poppe noted. Health plan sponsors should work with their insurers or third-party administrators to alleviate the risks associated with opioid dependence by encouraging nonopioid pain-management approaches, she advised. Employers can:
- Cover and demand opioid-free options for employees.
- Ask provider networks what they are doing to reduce opioid use post-surgery.
- Educate employees about discussing alternative pain strategies with their doctor. Pacira'sPlanAgainstPain website offers resources.
- Change benefit designs to steer employees to surgeons and facilities using alternatives to opioids
"To stem widespread opioid abuse, state actors and employers must urge insurers to remove barriers to care, including prior authorization for medication-assisted treatment (MAT) and nonopioid treatments for pain management," Caleb H. Randall-Bodman, a senior analyst for public affairs with Forbes Tate Partners in Washington, D.C., said in an e-mail.
"Patients, especially those in great need, will take the most affordable and accessible treatment available. As such, the epidemic will not end until patients have access to 1) affordable, comprehensive pain management, and 2) comprehensive treatment for substance use disorders," said Randall-Bodman, who works with the American Medical Association's taskforce to reduce opioid abuse.
SOURCE: Miller, S (28 November 2017) "Employers take steps to address opioid crisis" (Web Blog Post). Retrieved from https://www.shrm.org/resourcesandtools/hr-topics/benefits/pages/steps-to-address-opioid-crisis.aspx
The Opioid Epidemic and Medicaid’s Role in Facilitating Access to Treatment
The Kaiser Family Foundation has released the key findings in Medicaid's role in the opioid epidemic. Get the facts, statistics, and visual charts here.
Key Findings
In 2016, 1.9 million nonelderly adults in the United States had an opioid addiction. Medicaid covers 4 in 10 nonelderly adults with opioid addiction. This brief examines Medicaid’s role in facilitating access to treatment for opioid addiction. Key findings include:
- Among nonelderly adults with opioid addiction, those with Medicaid were twice as likely as those with private insurance or no insurance to have received treatment in 2016.
- Medicaid facilitates access to treatment by covering numerous inpatient and outpatient treatment services, as well as medications prescribed as part of medication-assisted treatment.
- States use Medicaid Section 1115 waivers and other program authorities to expand treatment options for enrollees with opioid addiction.
While additional states expanding Medicaid could increase coverage and access, support for new work and premium requirements could impose barriers to obtaining and maintaining Medicaid coverage that may compromise efforts to address the opioid crisis.
Introduction
The opioid epidemic continues to escalate, with 1.9 million nonelderly adults having an opioid addiction in 2016.1 Opioid addiction is often associated with comorbid physical and mental health conditions and high levels of health care services utilization. These issues have worsened throughout the past decade as the opioid epidemic has escalated. In 2016, there were 42,249 opioid overdose deaths in the United States, more than quadruple the number in 2001, and the number of deaths from heroin and fentanyl have surpassed the number due to prescription opioids. The Trump administration has stated that addressing the opioid epidemic is a key priority.
Medicaid has historically filled critical gaps in responding to public health crises, such as the AIDS epidemic in the 1980s, the Flint water crisis, and numerous natural disasters since the program originated. As with these other public health crises, Medicaid helps to address the opioid epidemic by providing access to coverage and necessary health care. The program covers a disproportionate share of individuals with opioid addiction and facilitates access to numerous treatment services. Additionally, as of February 2018, 33 states have adopted the Medicaid expansion, with enhanced federal funding, to cover adults up to 138% of the federal poverty level ($16,753/year for an individual in 2018). All Medicaid expansion benefit packages must include behavioral health services, including mental health and substance use disorder services, which has increased access to care for many people with opioid addiction.
Based on data from the 2016 National Survey on Drug Use and Health, this brief describes nonelderly adults with opioid addiction, including their demographic characteristics and insurance statuses, and compares receipt of various treatment services among those with Medicaid to those with private insurance and those who are uninsured. It also describes Medicaid financing for opioid treatment and the ways in which Medicaid promotes access to treatment for enrollees with opioid addiction.
Characteristics of Nonelderly Adults with Opioid Addiction
Individuals with opioid addiction are predominantly white, male, and young. In 2016, nearly 3 in 4 (74%) nonelderly adults with opioid addiction were white (Figure 1). Those with opioid addiction were also more likely to be male (58%), although the epidemic has touched an increasingly large share of women in recent years, including many pregnant women.2,3 Additionally, nearly half (48%) were between ages 18 and 34, and another one-third (32%) were between ages 35 and 49. This age distribution is comparable to those for other types of addiction, including addictions to both drugs and alcohol, which generally affect young adults more than they affect other age groups.4

Figure 1: Race, Gender, and Age of Nonelderly Adults with Opioid Addiction, 2016
The majority of nonelderly adults with opioid addiction are employed, but many have low incomes. In 2016, nearly 6 in 10 (56%) were employed; however, there was wide variability with regard to the types of jobs and industries in which they work, their salaries, and the number of hours they worked each week (Figure 2). Of those who were employed, about 7 in 10 (72%) reported working at a full-time job during the previous week.5 One in ten were unemployed and an additional 13% were unable to work because of a disability, reflecting the complicated health needs of individuals with opioid addiction, many of whom may have developed an addiction to opioids after using opioids to treat their chronic pain.6 Adults with opioid addiction are also more likely than other adults to have many other health conditions, including hepatitis, HIV, and mental illness,7 all of which may hinder their ability to work. As a result of these and other factors, more than half of nonelderly adults with opioid addiction had low incomes in 2016, and over a quarter (28%) lived below the poverty line (Figure 2).

Figure 2: Employment Status and Income of Nonelderly Adults with Opioid Addiction, 2016
Medicaid covers a disproportionate share of nonelderly adults with opioid addiction, and an even greater share of those with low incomes. In 2016, nearly 4 in 10 (38%) were covered by Medicaid and a similar share (37%) had private insurance. Approximately 1 in 6 (17%) was uninsured (Figure 3). Low-income nonelderly adults with opioid addiction are typically less likely than adults with higher incomes to have jobs that offer health insurance.8 In 2016, over half (55%) were covered by Medicaid, while only 13% had private insurance. Nearly 1 in 4 (24%) were uninsured (Figure 3), although if they lived in states that expanded Medicaid, they would likely be eligible for coverage.

Figure 3: Insurance Status of Nonelderly Adults with Opioid Addiction, 2016
Utilization of Opioid Addiction Treatment Services
Overall receipt of treatment for opioid addiction is low. In 2016, fewer than 3 in 10 (29%) adults with opioid addiction received any treatment for their addiction (Figure 4).9 Opioid addiction treatment can be delivered in an inpatient or outpatient setting and can be provided in numerous types of facilities, including hospitals, drug or alcohol rehabilitation facilities (for either inpatient or outpatient services), mental health centers, or private doctors’ offices. Depending on the severity of their addictions, some patients begin in an inpatient facility and then later transition to an outpatient setting, while others require only outpatient treatment. Overall, in 2016, 16% of nonelderly adults with opioid addiction received inpatient treatment, while 25% received outpatient treatment.

Figure 4: Past-Year Opioid Addiction Treatment Among Nonelderly Adults with Opioid Addiction by Insurance Status, 2016
Among nonelderly adults with opioid addiction, those with Medicaid are significantly more likely than those with private insurance or those who are uninsured to receive treatment. In 2016, those with Medicaid were twice as likely as those with private insurance or no insurance to receive any treatment for their addiction (43% vs. 21% and 23%). Nearly a quarter of adults with opioid addiction who had Medicaid coverage received inpatient care, while nearly 4 in 10 received outpatient care. In contrast, just over 1 in 10 (13%) of those with private insurance received any inpatient treatment and only 17% received any outpatient treatment. Those who were uninsured received treatment at rates similar to those with private insurance. These differences in utilization highlight the significant role Medicaid plays in increasing access to treatment.

Figure 5: Past-Year Outpatient Addiction Treatment Among Nonelderly Adults with Opioid Addiction by Insurance Status, 2016
Adults with opioid addiction who were covered by Medicaid were significantly more likely to have received treatment at an outpatient rehabilitation center or at an outpatient mental health center than those with private insurance or those who were uninsured (Figure 5). In 2016, adults with opioid addiction covered by Medicaid were three times more likely to have received treatment at these facilities than privately insured or uninsured adults. At the same time, utilization of services at private physician’s offices did not differ significantly across the three groups. Higher rates of utilization of outpatient treatment services by those with Medicaid may reflect the greater push for outpatient community-based behavioral health treatment in recent decades.10
Medicaid’s Role in Covering Opioid Addiction Treatment Services
State Medicaid programs cover numerous addiction treatment services that fit into several state plan categories, including outpatient treatment, inpatient treatment, prescription drugs, and rehabilitation. The standard of care for opioid addiction is medication-assisted treatment (MAT), which combines one of three medications (methadone, buprenorphine, or naltrexone) with counseling and other support services. All state Medicaid programs cover at least one medication used as part of MAT,11 and most cover all three of these medications. State Medicaid programs also cover many counseling and other support services, delivered either as part of MAT or separately. Most of these services are delivered at state option and include detoxification, intensive outpatient treatment, psychotherapy, peer support, supported employment, partial hospitalization, and inpatient treatment.12
Several policy changes have allowed states to obtain waivers to allow Medicaid funding of substance use treatment services at institutions for mental disease (IMDs). Federal law has historically prohibited Medicaid payments for services provided to adults age 21-64 in IMDs as a way to preserve state financing of these services. However, in April 2016, CMS issued final Medicaid managed care regulations that allow federal matching funds for managed care capitation payments for services in an IMD for up to 15 days in a month in lieu of services covered under the state plan and at the enrollee’s option.13 Additionally, in July 2015, the Centers for Medicare & Medicaid Services (CMS) released guidance stating that states could request federal funding for substance use disorder services delivered to nonelderly adults in IMDs through Section 1115 demonstration waivers. On November 1, 2017, CMS issued revised guidance that continues to allow states to seek Section 1115 waivers to pay for services provided in IMDs, including substance use disorder services. A number of states have sought waivers of the IMD exclusion specifically to expand treatment options for substance use disorder services. As of March 2018, CMS has approved waiver requests in 10 states to provide substance use disorder services in an IMD, and 10 states have waiver applications pending with CMS.14
Many states have also applied for other Medicaid Section 1115 behavioral health waivers focused on treating individuals with addiction, including opioid addiction. CMS has approved community-based benefit expansions proposed in Section 1115 waivers, which enable states to provide additional services to individuals with addiction, such as supportive housing, supported employment (such as job coaching), and peer recovery coaching. Additionally, CMS has approved waivers that allow states to expand Medicaid eligibility to cover additional populations with behavioral health needs, to provide home and community-based services, and to implement certain delivery system reforms, such as physical and behavioral health integration and alternative payment models.
Because of the large number of Medicaid enrollees with opioid addiction and the breadth of treatment services that Medicaid covers, Medicaid finances a substantial proportion of addiction treatment. In 2014, Medicaid financed 21% of all addiction treatment, which was more than the share covered by all private insurers combined (18%). Nine percent of all spending on addiction treatment came from out-of-pocket payments (Figure 6).15

Figure 6: Proportion of Total Spending on Addiction Treatment Services in 2014, by Payer
Looking Ahead
Medicaid plays a major role in facilitating access to inpatient and outpatient treatment services for individuals with opioid addiction. Nonelderly adults with Medicaid were more likely than those without insurance to receive various types of opioid addiction treatment and had better access to treatment than those with private insurance. Furthermore, despite the IMD payment exclusion, individuals with Medicaid were more likely than privately insured individuals to receive inpatient treatment.
As the opioid epidemic continues to worsen, particularly as fentanyl has become more pervasive,16 states are increasingly looking to Medicaid to expand treatment options to stem the crisis. In addition to covering MAT medications and numerous other treatment services, states are seeking waivers to allow payment for opioid treatment services provided in IMDs, to expand coverage of community-based benefits to support treatment and recovery, and better integrate behavioral health services, including substance use disorder services, with physical health services.
Non-expansion states can improve access to treatment by expanding Medicaid, which would enable them to cover many people with opioid addiction who are currently uninsured. At the same time, using 1115 waivers to impose new requirements in Medicaid, including work requirements and premiums, could compromise efforts to address the opioid epidemic. Although some states exempt people in addiction treatment from work requirements and other states count treatment as work hours, other states do not have such exemptions. Additional reporting requirements coupled with new premium requirements may also make it more difficult for eligible individuals to enroll in Medicaid and for those currently enrolled to keep their coverage. Utilization of treatment by adults with an opioid addiction is already low; imposing new barriers to obtaining and maintaining Medicaid could further impede those battling opioid addiction from getting the care they need.
This article was brought to you from the Kaiser Family Foundation on April 11,2018.