

I Have Life Insurance Through My Employer. Why Do I Need Another Policy?
Life Happens in a Heartbeat - Stay Prepared With Saxon Life Insurance.
Although it is a subject no one wants to talk about, Life Insurance may be one of the best purchases you ever make.
Have you considered what would happen if you were not there to take care of your loved ones? Life insurance plans are about preparing for the unexpected. While nothing can replace you, having Life Insurance helps ensure that your family and loved ones would be financially stable if anything was to ever happen to you. Check out this article from Life Happens on the importance of obtaining Life Insurance - even if it's already offered through your employer.
One of the perks of having a full-time job with a good company is the benefits package that comes with it. Often, those benefits include life insurance coverage, which is great. And everyone who can get life insurance at work should definitely take it, as there are many advantages to company-funded life insurance, also known as group life insurance. These advantages include:
1. Easy qualification. Often, enrollment into group life insurance is automatic. That means everyone qualifies, as there is no medical exam required. So people who have preexisting health conditions, like diabetes or previous heart attack, can get life insurance at work, and may get a better rate compared with what an individual life insurance policy might cost them.
2. Lower costs. Employers’ insurance plans tend to be paid for or subsidized by the company, giving you life insurance at a low cost or even free. You may even have the option to buy additional coverage at low rates. Costs tend to be lower for many people because with group plans, the cost per individual goes down as the plan enlarges.
3. Convenience. It’s easy to subscribe to an employer’s life insurance plan without much effort on your part and if a payment is required, it’s easily deducted from your paycheck in much the same way as your medical costs are deducted.
These are all great advantages, but are these the only considerations that matter when it comes to life insurance? The answer, of course, is no.
Life insurance should first and foremost fit the purpose—it should meet your needs.
Life insurance should first and foremost fit the purpose—it should meet your needs. And the primary purpose of life insurance is to care for those left behind in the event of your death. With group life insurance, it’s often set at one or two times your annual salary, or a default amount such as $25,000 or $50,000. While this sounds like a lot of money, just think of how long that would last your loved ones. What would they do once that ran out?
There are several other disadvantages to relying on group insurance alone:
1. If your job situation changes, you’ll lose your coverage. Whether the change results from being laid off, moving from full-time to part-time status or leaving the job, in most cases, an employee can’t retain their policy when they leave their job.
2. Coverage may end when you retire or reach a specific age. Many people tend to lose their insurance coverage when they continue working past a specified age or when they retire. This means losing your insurance when you need it most.
3. Your employer can change or terminate the coverage. And that can be without your consent, since the contract is between your employer and the insurer.
4. Your options are limited. This type of coverage is not tailored to your specific needs. Furthermore, you may not be able to buy as much coverage as you need, leaving you exposed.
Importance of Buying a Separate Life Insurance Policy
It’s for these reasons you should get an individual life insurance policy that you personally own, in addition to any group life insurance you have. Individual life insurance plans offer superior benefits, and regardless of your employer or employment status, they remain in place and can be tailored to meet your needs and circumstances.
Most importantly, an individual life insurance policy will fit the purpose for which you purchase it—to ensure your dependents continue to have the financial means to keep their home and lifestyle in the unfortunate event that you’re no longer there to care for them.
Don't wait to protect your livelihood. Set up an appointment with one of our life insurance specialists here at Saxon by clicking this link.
Source:
Medina F. (19 June 2017). "I Have Life Insurance Through My Employer. Why Do I Need Another Policy?" [Web blog post]. Retrieved from address https://www.lifehappens.org/blog/i-have-life-insurance-through-my-employer-why-do-i-need-another-policy/

More than Half of Uninsured People Eligible for Marketplace Insurance Could Pay Less for Health Plan than Individual Mandate Penalty
Things are not looking up for the uninsured. Pay less and reach out to your health insurance professionals today. Want more facts? Check out this blog article from Kaiser Family Foundation.
A new Kaiser Family Foundation analysis finds that more than half (54% or 5.9 million) of the 10.7 million people who are uninsured and eligible to purchase an Affordable Care Act marketplace plan in 2018 could pay less in premiums for health insurance than they would owe as an individual mandate tax penalty for lacking coverage.
Within that 5.8 million, about 4.5 million (42% of the total) could obtain a bronze-level plan at no cost in 2018, after taking income-related premium tax credits into account, the analysis finds.
Most people without insurance who are eligible to buy marketplace coverage qualify for subsidies in the form of tax credits to help pay premiums for marketplace plans (8.3 million out of 10.7 million). Among those eligible for premium subsidies, the analysis finds that 70 percent could pay less in premiums than what they’d owe as a tax penalty for lacking coverage, with 54 percent able to purchase a bronze plan at no cost and 16 percent contributing less to their health insurance premium than the tax penalty they owe.
Among the 2.4 million uninsured, marketplace-eligible people who do not qualify for a premium subsidy, 2 percent would be able to pay less for marketplace insurance than they’d owe for their 2018 penalty, the analysis finds.
The Affordable Care Act’s individual mandate requires that most people have health coverage or be subject to a tax penalty unless they qualify for certain exemptions. The individual mandate is still in effect, though Congress may consider repealing it as part of tax legislation.
Consumers can compare their estimated 2018 individual mandate penalty with the cost of marketplace insurance in their area with KFF’s new Individual Mandate Penalty Calculator.
The deadline for ACA open enrollment in most states is Dec. 15, 2017.
You can read the original article here.
Source:
Kaiser Family Foundation (9 November 2017). "ANALYSIS: More than Half of Uninsured People Eligible for Marketplace Insurance Could Pay Less for Health Plan than Individual Mandate Penalty" [Web blog post]. Retrieved from address https://www.kff.org/health-reform/press-release/analysis-more-than-half-of-uninsured-people-eligible-for-marketplace-insurance-could-pay-less-for-health-plan-than-individual-mandate-penalty/

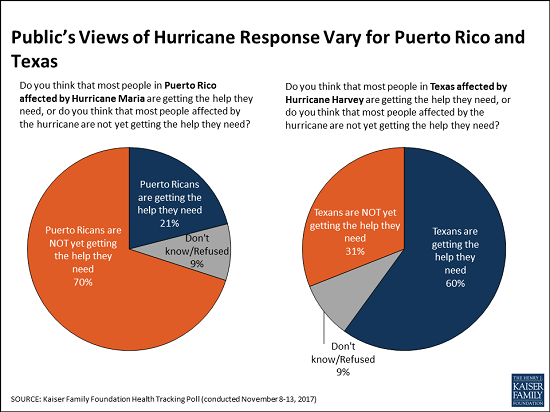
Two Months After Hurricane Maria, A Growing Majority Of Americans Say Puerto Ricans are Not Yet Getting the Help They Need
Two months after Hurricane Maria struck Puerto Rico, a growing majority of Americans say that Puerto Ricans affected by the devastating storm are not yet getting the help they need, the November Kaiser Family Foundation Tracking Poll finds.
This month, 70 percent of the public say that people in Puerto Rico are not yet getting the help they need, up from 62 percent in October 2017. These perceptions vary by party, and half of Republicans (52%) now say Puerto Ricans aren’t yet getting needed help, up significantly from October (38%).
When asked whether the federal government is doing enough to restore electricity and access to food and water in Puerto Rico or not, a majority of the public (59%) says the federal government is not doing enough, up from 52 percent in October. Most Democrats (86%) and independents (59%) say the federal government is not doing enough, but most Republicans (63%) say it is doing enough.
In contrast, Americans see the recovery efforts in Texas following Hurricane Harvey in late August progressing more positively. Most (60%) of the public says Texans are getting the help they need, twice the share (31%) who say Texans aren’t yet getting needed help.
The poll finds similar shares of Americans they are closely following news about recovery efforts in Puerto Rico (63%) and in Texas (58%). Democrats are somewhat more likely to report closely following news about the Puerto Rico recovery (75%) than are independents (61%) and Republicans (54%). In contrast, there are no partisan differences for those following news about Texas.
Designed and analyzed by public opinion researchers at the Kaiser Family Foundation, the poll was conducted from November 8 – 13, 2017 among a nationally representative random digit dial telephone sample of 1,201 adults. Interviews were conducted in English and Spanish by landline (415) and cell phone (786). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
You can read the original article here.
Source:
Kaiser Family Foundation (20 November 2017). "Two Months After Hurricane Maria, A Growing Majority Of Americans Say Puerto Ricans are Not Yet Getting the Help They Need" [Web blog post]. Retrieved from address https://www.kff.org/other/press-release/poll-two-months-after-hurricane-maria-a-growing-majority-of-americans-say-puerto-ricans-are-not-ye-getting-the-help-they-need/
SaveSave
Pressure Builds To Cut Medicare Patients In On Prescription Deals
In this article from Kaiser Health News, the stupendous rise of prescription costs is finally addressed. What steps are being taken to reduce costs for Medicare patients? Find out below.
Medicare enrollees, who have watched their out-of-pocket spending on prescription drugs climb in recent years, might be in for a break.
Federal officials are exploring how beneficiaries could get a share of certain behind-the-scenes fees and discounts negotiated by insurers and pharmacy benefit managers, or PBMs, who together administer Medicare’s Part D drug program. Supporters say this could help enrollees by reducing the price tag of their prescription drugs and slow their approach to the coverage gap in the Part D program.
The Centers for Medicare & Medicaid Services (CMS) could disclose the fees to the public and apply them to what enrollees pay for their drugs. However, there’s no guarantee that such an approach would be included in a proposed rule change that could land any day, according to several experts familiar with the discussions.
“It’s obvious something has to be done about this. This is causing higher drug prices for patients and taxpayers,” Rep. Earl “Buddy” Carter (R-Ga.), a pharmacist, said this week.
While Medicare itself cannot negotiate drug prices, the health insurers and PBMs have long been able to negotiate with manufacturers who are willing to pay rebates and other discounts so their products win a good spot on a health plan’s list of approved drugs.
Federal officials described these fees in a January fact sheet as direct and indirect remuneration, or DIR fees.
In recent years, pharmacies and specialty pharmacies have also begun paying fees to PBMs. These fees, which are different than the rebates and discounts offered by manufacturers, can be controversial, in part, because they are retroactive or “clawed back” from the pharmacies.
The controversy is also part of the reason advocates, such as pharmacy organizations, have lobbied for this kind of policy change.
PBMs have long contended that they help contain costs and are improving drug availability rather than driving up prices.
Pressure has been building for the administration to take action. Earlier this year, the federal agency’s fact sheet set the stage for change, describing how the fees kept Medicare Part D monthly premiums lower but translated to higher out-of-pocket spending by enrollees and increased costs to the program overall.
In early October, Carter led a group of more than 50 House members in a letter urging Medicare to dedicate a share of the fees to reducing the price paid by Part D beneficiaries when they buy a drug. Also in the House, Rep. Morgan Griffith (R-Va.) introduced a related bill.
On the Senate side, Chuck Grassley (R-Iowa) and 10 other senators sent a letter in July to CMS Administrator Seema Verma as well as officials at the Department of Health and Human Services asking for more transparency in the fees — which could lead to a drop in soaring drug prices if patients get a share of the action.
A response from Verma last month notes that the agency is analyzing how altering DIR requirements would affect Part D beneficiary premiums — a key point that muted previous political conversations.
But advocates say the tone of discussions with the agency and on Capitol Hill have changed this year. That’s partly because Medicare beneficiaries have become more vocal about their rising out-of-pocket costs, increasing scrutiny of these fees.
Ellen Miller, a 70-year-old Medicare enrollee in New York City’s borough of Queens, sent a letter to the Trump administration demanding lower drug prices. Miller’s prescription prices went up this year, sending her into the Medicare “doughnut hole” by April, compared with October in 2016. With coverage, Miller pays about $200 a month for several prescriptions that help her cope with COPD, or chronic obstructive pulmonary disease, as well as another chronic illness.
In the doughnut hole, where coverage drops until catastrophic coverage kicks in, her out-of-pocket costs climb to $600 a month.
It’s “ridiculous, and that doesn’t count my medical bills,” Miller said.
The number of Medicare Part D enrollees with high out-of-pocket costs, like Miller, is on the rise. And in 2015, 3.6 million Medicare Part D enrollees had drug spending above the program’s catastrophic threshold of $7,062, according to a report released this week by the Kaiser Family Foundation. (Kaiser Health News is an editorially independent program of the foundation.)
Supporters of the rule change say making the fees more transparent and applying them to what enrollees pay would provide relief for beneficiaries like Miller.
The Pharmaceutical Care Management Association (PCMA), which represents the PBMs who negotiate the rebates and discounts, says changing the fees would endanger the Part D program.
“In Medicare Part D, you have one of the most successful programs in health care,” said Mark Merritt, president and chief executive of PCMA. “Why anybody would choose to destabilize the program is beyond me.”
CMS declined to comment on a vague reference to a pending rule change, which was posted in September.
For now, though, according to the CMS fact sheet, the fees pose two compounding problems for seniors and the agency:
- Enrollees pay more out-of-pocket for each drug, causing them to reach the program’s coverage gap quicker. In 2018, the so-called doughnut hole begins once an enrollee and the plan spends $3,750 and ends at $5,000 out-of-pocket, and then catastrophic coverage begins.
- Medicare, thus taxpayers, pays more for each beneficiary. Once enrollees reach the threshold for catastrophic coverage, Medicare pays the bulk cost of the drugs.
CVS Health, one of the nation’s top three PBMs, released a statement in February calling the fees part of a pay-for-performance program that helps improve patient care. The fees, CVS noted, are fully disclosed and help drive down how much Medicare pays plans that help run the program.
“CVS Health is not profiting from this program,” the company noted.
Express Scripts, also among the nation’s top three PBMs, agreed that the fees lower costs and give incentives for the pharmacies to deliver quality care. As for criticism from the pharmacies, Jennifer Luddy, director of corporate communications for the company, said, “We’re not administering fees in a way that penalizes a pharmacy over something they cannot control.”
Regardless, even if a rule is changed or a law is passed, there is some question as to how easily the fees can translate into lower costs for seniors, in part because the negotiations are so complicated.
When the Medicare Payment Advisory Commission, which provides guidance to Congress, discussed the negotiations in September, Commissioner Jack Hoadley thanked the presenters and said, “In my eyes, what you’ve revealed is a real maze of financial … entanglements.”
Tara O’Neill Hayes, deputy director of health care policy at the conservative American Action Forum, said passing on the discounts and fees to beneficiaries when they buy the drug could be difficult because costs crystallize only after a sale has occurred.
“They can’t be known,” said Hayes, who created an illustration of the negotiations.
“There’s money flowing many different ways between many different stakeholders,” Hayes said.
Source:
Tribble S. (10 November 2017). "Pressure Builds To Cut Medicare Patients In On Prescription Deals" [Web blog post]. Retrieved from address https://khn.org/news/pressure-builds-to-cut-medicare-patients-in-on-prescription-deals/

Taking A Page From Pharma’s Playbook To Fight The Opioid Crisis
From Kaiser Health News, here is the latest: an interview with Dr. Mary Meengs, medical director at the Humboldt Independent Practice Association, on curbing opioid addiction through the reduction of prescription painkillers.
Dr. Mary Meengs remembers the days, a couple of decades ago, when pharmaceutical salespeople would drop into her family practice in Chicago, eager to catch a moment between patients so they could pitch her a new drug.
Now living in Humboldt County, Calif., Meengs is taking a page from the pharmaceutical industry’s playbook with an opposite goal in mind: to reduce the use of prescription painkillers.
Meengs, medical director at the Humboldt Independent Practice Association, is one of 10 California doctors and pharmacists funded by Obama-era federal grants to persuade medical colleagues in Northern California to help curb opioid addiction by altering their prescribing habits.
She committed this past summer to a two-year project consisting of occasional visits to medical providers in California’s most rural areas, where opioid deaths and prescribing rates are high.
“I view it as peer education,” Meengs said. “They don’t have to attend a lecture half an hour away. I’m doing it at [their] convenience.”
This one-on-one, personalized medical education is called “academic detailing” — lifted from the term “pharmaceutical detailing” used by industry salespeople.
Detailing is “like fighting fire with fire,” said Dr. Jerry Avorn, a Harvard Medical School professor who helped develop the concept 38 years ago. “There is some poetic justice in the fact that these programs are using the same kind of marketing approach to disseminate helpful evidence-based information as some [drug] companies were using … to disseminate less helpful and occasionally distorted information.”
Recent lawsuits have alleged that drug companies pushed painkillers too aggressively, laying the groundwork for widespread opioid addiction.
Avorn noted that detailing has also been used to persuade doctors to cut back on unnecessary antibiotics and to discourage the use of expensive Alzheimer’s disease medications that have side effects.
Kaiser Permanente, a large medical system that operates in California, as well as seven other states and Washington, D.C., has used the approach to change the opioid-prescribing methods of its doctors since at least 2013. (Kaiser Health News is not affiliated with Kaiser Permanente.)
In California, detailing is just one of the ways in which state health officials are attempting to curtail opioid addiction. The state is also expanding access to medication-assisted addiction treatment under a different, $90 million grant through the federal 21st Century Cures Act.
The total budget for the detailing project in California is less than $2 million. The state’s Department of Public Health oversees it, but the money comes from the federal Centers for Disease Control and Prevention through a program called “Prevention for States,” which provides funding for 29 states to help combat prescription drug overdoses.
The California doctors and pharmacists who conduct the detailing conversations are focusing on their peers in the three counties hardest hit by opioid addiction: Lake, Shasta and Humboldt.
They arrive armed with binders full of facts and figures from the CDC to help inform their fellow providers about easing patients off prescription painkillers, treating addiction with medication and writing more prescriptions for naloxone, a drug that reverses the toxic effects of an overdose.
“Academic detailing is a sales pitch, an evidence-based … sales pitch,” said Dr. Phillip Coffin, director of substance-use research at San Francisco’s Department of Public Health — the agency hired by the state to train the detailers.
In an earlier effort, Coffin said, his department conducted detailing sessions with 40 San Francisco doctors, who have since increased their prescriptions of naloxone elevenfold.
“One-on-one time with the providers, even if it was just three or four minutes, was hugely beneficial,” Coffin said. He noted that the discussions usually focused on specific patients, which is “way more helpful” than talking generally about prescription practices.
Meengs and her fellow detailers hope to make a dent in the magnitude of addiction in sparsely populated Humboldt County, where the opioid death rate was the second-highest in California last year — almost five times the statewide average. Thirty-three people died of opioid overdoses in Humboldt last year.
One recent afternoon, Meengs paid a visit during the lunch hour to Fortuna Family Medical Group in Fortuna, a town of about 12,000 people in Humboldt County.
“Anybody here ever known somebody, a patient, who passed away from an overdose?” Meengs asked the group — a physician, two nurses and a physician assistant — who gathered around her in the waiting room, which they had temporarily closed to patients.
“I think we all do,” replied the physician, Dr. Ruben Brinckhaus.
Brinckhaus said about half the patients at the practice have a prescription for an opioid, anti-anxiety drug or other controlled substance. Some of them had been introduced to the drugs years ago by other prescribers.

Dr. Ruben Brinckhaus says his small family practice in Fortuna, Calif., has been trying to wean patients off opiates. (Pauline Bartolone/California Healthline)
Meengs’ main goal was to discuss ways in which the Fortuna group could wean its patients off opioids. But she was not there to scold or lecture them. She asked the providers what their challenges were, so she could help them overcome them.
Meengs will keep making office calls until August 2019 in the hope that changes in the prescribing behavior of doctors will eventually help tame the addiction crisis.
“It’s a big ship to turn around,” said Meengs. “It takes time.”
Source:
Bartolone P. (14 November 2017). "Taking A Page From Pharma’s Playbook To Fight The Opioid Crisis" [Web blog post]. Retrieved from address https://khn.org/news/taking-a-page-from-pharmas-playbook-to-fight-the-opioid-crisis/
SaveSave

Data transparency, debt consolidation and ID protection lead open enrollment wish list
In the thick of open enrollment season, savvy employers and benefit advisers have eased the onslaught of information with complex benefit jargon by spreading out employee sign-up before the mad fall rush. Employee Benefit Adviser spoke with Jeffrey Faber, HUB International Midwest’s chief operating officer, to discuss how employers are urging employees to save with data transparency tools, use interactive services to learn about new benefits and to sign up for identity protection.
EBA: How is open enrollment going for you and your clients?
Faber: We’re in the middle of open enrollment season and we are trying to lock down the last-minute decisions our clients have. Predominantly our business is a renewal business.
Our large groups have made their decisions already but our smaller groups are just finding out what their renewals are from the major medical carriers. We have our hands full trying to make sense of it all. But open enrollment is the focus. This is absolutely our busiest time of year. From mid-August to Halloween, and even mid-November, it seems to be getting longer and longer every year with all the nuances our clients require.
EBA: How does this enrollment season differ from previous years? Is there confusion over the ACA’s status? Is there a greater emphasis on voluntary benefits?
Faber: On the repeal of Obamacare, a lot of those decisions have been made too late for our employers to really have to pivot and they are unaffected largely by the executive orders and the talk from Congress. Of course, there's the specter that Congress will act and make a decision in the next couple of weeks, but that impact would probably be a 2019 event instead of a 2018 event.
On the voluntary benefits side, our clients are asking for financial and holistic tools to meet the employees where they live in regard to student loans, tuition assistance and debt consolidation services. ID theft has been a big conversation point in the last three or four months and has been heightened by the Equifax breach, but it started three years ago with the Target breach. A lot of employers want to understand their role in their employee’s lives,

And for voluntary benefits, most of our customers are moving to the consumer-driven model with higher deductibles, so accident insurance, critical injury insurance, and hospitalization – those are all nice bolt-on benefits for the medical benefits they have. It almost allows the employee to self-insure their own health. And HSAs and HRAs are still popular. We see a large uptick year over year over year.
EBA: Any other trends for this year’s open enrollment?
Faber: A few years ago, we joked that overall enrollment was the HR Super Bowl. It happened once a year, it was a three hour event with a bunch of commercials and no one really talked about it a week or two later.
Our clients have asked, what can we do the other 11 months a year? We have seen an increase in requests for interactive PDFs, on-demand video, and interactive guides directing folks to microsites or apps on their phone. We introduce these in April, May or June and if the employee needs this, they don't have to go back into their memory bank and access it, they can get it online. It is that year round learning that engages the customer.
EBA: Is this because employees are bombarded with information during open enrollment?
Faber: Yes and no. There is a lot of information that is required and that is distributed this time of year and there are a lot of decision points that they have to make for themselves and the benefit of their families. We put in place decision helping tools like Jellyvision’s ALEX and some other proprietary tools, that can help employees better make decisions.
But I think it is more toward trying to be a circuit breaker in an employee's head when they are accessing healthcare. That makes them stop and check, “Is this in network, do I have to get pre-authorization? How do I check for a lower cost across the street from a benefit provider?”
These things come out of the workshops this time of year, but if you are not hitting employees where they live at the time of use, you are missing those opportunities for significant cost savings. And not on just on the employer side but the employee side especially with high-deductible plans.
EBA: Is data transparency a big push for this open enrollment season?
Faber: Yes, especially when you consider that standalone imaging facilities are three to eight times less expensive than an in-house hospital facility. Employees need to understand that they will pay 100% of that cost until they meet that deductible in that consumer-driven plan, so there is every effort being made to make sure the employee is checking those transparency tools.
At open enrolment time, we make every effort to employees in the room to ID the nearest urgent care and ER facility, to write those down on a note card and put it in the visor of their car. So, they know at the moment of crisis to know where those places are and make decisions ahead of time.
EBA: Accountants say that from January to April 15, they don't see their families. Is it the same for you during open enrollment?
Faber: (Laughs) I grew up in an accounting family and I can attest to that. It is all hands on deck but our goal is to help clients get their decisions out of the way in Q1 and Q2. We try to help them with decisions that don't require immediacy and don’t have to be made right away, like life and disability insurance, and voluntary and wellness benefits. You can make a lot of those decisions in April, May and June.
Source:
Albinus P. (30 October 2017). "Data transparency, debt consolidation and ID protection lead open enrollment wish list" [Web blog post]. Retrieved from address https://www.employeebenefitadviser.com/news/data-transparency-debt-consolidation-and-id-protection-lead-open-enrollment-wish-list-says-hub-international-midwest-coo-jeffrey-faber?feed=00000152-1387-d1cc-a5fa-7fffaf8f0000
SaveSave
SaveSaveSaveSave

5 ways to empower employees to make smart healthcare choices
As an employer, it's important to help your employees out when you can - especially when it comes to making smart healthcare choices. In this article from Employee Benefit Advisor, Anne Stowell lists five different ways to empower your employees.
As uncertainty in healthcare policy lingers, creating a benefits package with real value for both employers and employees can seem increasingly complex and difficult to achieve. Striving to provide the right care services — ones that are easy for employees to use, and designed to increase engagement in their care while being mindful of costs — is undoubtedly a tricky balancing act.
So how can employers engage to help employers offer benefits that have real and lasting value, while empowering employees to make smart care choices? Here are five tips:
1) Learn your clients’ hot buttons. Value is one of the most important factors employers consider when shopping for benefits. Rise Broadband, for example, the largest fixed wireless service provider in the U.S., has a large number of employees working in the field to service remote customers. Accessing healthcare when employees are on the road was a real challenge. Jennifer Iannapollo, the company’s director of HR, says their telehealth benefit provides employees with real value, and was the clear answer for this Colorado-based employer.

Bloomberg/file photo
2) Recognize empowerment comes with confidence. Employees won’t use what they aren’t sure of. Iannapollo also was careful to choose a telehealth platform that focused on quality. “Some people needed reassurance about who would be treating them and how they would know their medical history. We reassured them that their medical records and history are collected when they register and that the physicians are all board certified and average 20 years of experience. That provided them with peace of mind,” she says. Security practices and certifications can also add a level of comfort, and are something advisers should keep in mind in their recommendations for any product to employers.
3) Remind employees to take charge of their own healthcare destiny. A recent Teladoc survey of more than 300 employers found that a whopping 66% stated that lack of benefit awareness negatively affects employee engagement with health benefits. That’s where advisers have an opportunity to shine by emphasizing the need to communicate and educate employees not just during benefit season, but whenever/wherever their moment of need might be. “Surround sound” reminders are proven to help. One creative idea that Rise Broadband adopted was dashboard stickers that help field technicians’ keep available benefits top of mind.
4) Combat “vendor fatigue.” Employers are inundated by the staggering number of benefits options, not to mention trying to manage countless vendors that all have a piece of the benefits package puzzle. Advisers can help clear the confusion by working closely with their clients to help them source solutions that meet a broad array of needs for everything from sinus infections to behavioral health to getting second opinions.
5) Educate employers that employee engagement is a winning strategy. Advisers agree with us that technology that provides real-time information for decision-making and access to quality healthcare for employees provides real value. Reed Smith, SVP/employee benefits practice leader, CoBiz Insurance, in Denver, believes that like other disruptive innovation (think Apple and Amazon) that has transformed consumer interactions, engaged telehealth, when deployed effectively, can result in a happier, healthier and more involved employee, which means a healthier bottom line for the employer.
Source:
Stowell A. (8 November 2017). "5 ways to empower employees to make smart healthcare choices" [Web blog post]. Retrieved from address https://www.employeebenefitadviser.com/opinion/5-ways-to-empower-employees-to-make-smart-healthcare-choices
SaveSave

Employers prefer paper-based approach for open enrollment
Sure, technology is great, but can it ever live up to a face-to-face sit down? Let's take a look at the facts from Employee Benefit Advisor.
Fewer than half of businesses use technology to handle annual enrollment or manage time off, Affordable Care Act reporting or benefits changes during the year, according to a recent white paper by one of the nation’s leading ancillary benefits providers.
Citing a 2017 LIMRA report entitled “Convenient and Connected: Employers and Benefits,” Colonial Life highlighted several reasons why employers are resisting the digital age. They believe their organization isn’t big enough (32%), a technology solution is too expensive (24%), they don’t have enough staff (16%), in-person meetings are more engaging, or it’s the preference of their broker or plan administrator (tied at 15%).
In fact, Colonial Life post-enrollment surveys from 2009 to 2016 show that 98% of employees understand their benefits better through 1-to-1 benefits counseling and 95% describe the personalized attention they received as valuable.
Steven Johnson, vice president in premier markets and enrollment solutions at Colonial Life, was surprised by the prevalence of “manual and outdated ways.” However, he also understands the tendency to resist change— noting, for example, how some people still maintain landlines in spite of a reliance on smartphones for calls, text, e-mail, social media and GPS directions.

“Slow adoption of technology can be especially true in the workplace,” he says. “Heavy dependence of the fax machine at many workplaces still baffles me with so much advanced technology available to perform the job better, faster and cheaper.”
For those employers looking to add capabilities to their benefits technology programs, the report noted that LIMRA found most cited cost reduction (36%) or control of benefit data (35%). Rounding out the list was reduced staff time (32%), improved benefits communications (29%) and better employee experience (27%).
Among the features most sought after for either benefits administration systems, enrollment technology or both, LIMRA said low cost led the way (87%), followed by data security (86%), ease of use for employees (85%), it’s accessible all year (80%), employees re-enrolled annually or all insurance benefits are on the same platform (77% apiece).
Colonial Life stressed the importance of providing personalized resource materials, such as web content, e-mails and one-to-one meetings, as well as ample time for employees to make wise choices for themselves and dependents. Another recommendation was that insurance carriers make available benefits counselors to help guide employees through their decisions.
Johnson urged benefit brokers and advisers to help educate their clients on affordable enrollment technology solutions that will greatly enhance the experience for their employees while also reducing administrative burdens and challenges for employers and plan administrators.
“A trusted benefits adviser can share case study examples from companies of similar size and industry to illustrate the benefits of adopting a benefits admin solution for enrollment,” he says. In addition, he suggests that employee survey feedback can be shared to help advance the argument that “the overall experience is far better for those who’ve used technology to help them make their important benefits decisions.”
Source:
Shutan B. (13 November 2017). "Employers prefer paper-based approach for open enrollment" [Web blog post]. Retrieved from address https://www.employeebenefitadviser.com/news/employers-prefer-paper-based-approach-for-open-enrollment?brief=00000152-1443-d1cc-a5fa-7cfba3c60000
SaveSave
SaveSave

Some States Roll Back ‘Retroactive Medicaid,’ A Buffer For The Poor — And For Hospitals
From Kaiser Health News, let's take a look at the latest regarding Medicaid.
If you’re poor, uninsured and fall seriously ill, in most states if you qualify for Medicaid — but weren’t enrolled at the time — the program will pay your medical bills going back three months. It protects hospitals, too, from having to absorb the costs of caring for these patients.
But a growing number of states are rescinding this benefit known as “retroactive eligibility.” On Nov. 1, Iowa joined three states that have eliminated retroactive coverage for some groups of Medicaid patients since the Affordable Care Act passed. Each state had to secure approval by the federal government.
Retroactive eligibility has been a feature of Medicaid for decades, reflecting the program’s emphasis on providing a safety net for poor, disabled and other vulnerable people. In contrast to private insurance, determining Medicaid eligibility can be complex and the application process daunting, advocates say. A patient’s medical condition also may keep families from applying promptly for coverage.
All four states — Arkansas, Indiana and New Hampshire, in addition to Iowa — have expanded Medicaid under the health law, which allowed states to include adults with incomes up to 138 percent of the federal poverty level, or about $16,000 for one person. So, in theory, most adults are required to have insurance under the ACA. In practice, each state still has a significant number of uninsured, ranging from 5 to 8 percent of the population.
The retroactive coverage “can compensate for the sorts of errors and lapses that can so easily occur on the part of both the applicant and the government bureaucracy” that delay applications, said Gordon Bonnyman, staff attorney at the Tennessee Justice Center, a public interest law firm that represents low-income and uninsured residents.
State and federal officials say eliminating the retroactive coverage helps encourage people to sign up for and maintain coverage when they’re healthy rather than waiting until they’re sick to enroll. It also fits into federal officials’ efforts to make Medicaid, the federal-state program that provides health care for low-income adults and children, more like private insurance.
But consumer advocates and health care providers say the shift will saddle patients with hefty medical bills and leave hospitals to absorb more uncompensated care when patients can’t pay. Some worry this could be the start of a trend.
In Iowa, the change applies to just about anyone coming into Medicaid — except for pregnant women and children under age 1. The change will affect up to 40,000 residents annually and save the program more than $36 million a year.
“We’re making it a lot more likely that Medicaid-eligible members are going to incur significant medical debt,” said Mary Nelle Trefz, health policy associate at the Child & Family Policy Center in Des Moines, whose organization opposed the change.
When someone has a traumatic health event, the initial focus is to get them stabilized, not figure out how to pay for it, said MaryBeth Musumeci, associate director of the Program on Medicaid and the Uninsured at the Kaiser Family Foundation. (Kaiser Health News is an editorially independent program of the foundation.)
Patients may neglect to apply immediately for Medicaid, leaving them financially responsible for days or months of care they received before they got in their application, even though they may have been eligible for Medicaid all along.
That’s not the only issue, advocates say. Unlike the commercial insurance market where re-enrollment through someone’s employer is routine, Medicaid requires that beneficiaries’ eligibility be reassesed every year.
“People fall through the cracks,” said Andrea Callow, associate director of Medicaid initiatives at Families USA, a consumer advocacy group.
In addition, complications can arise for people who might need Medicaid coverage for long-term care services. “The criteria are complicated. For a layperson to find those criteria and figure out if they’re eligible” is challenging and they may need extra time, said Musumeci. Once patients have secured coverage, they may already have accrued hefty expenses.
Maybe so, but some people argue that a 90-day retroactive eligibility guarantee is counterproductive.
“We’re trying to get people to behave more responsibly, not less responsibly,” said Gail Wilensky, an economist who oversaw the Medicaid and Medicare programs in the early 1990s under President George H.W. Bush. “That is not the signal you’re sending” with three months of retroactive eligibility. A 30-day time frame is more reasonable, Wilensky said.
In contrast to Iowa, the waivers in Arkansas, Indiana and New Hamsphire generally apply only to adults who gained coverage under the law’s Medicaid expansion. (Indiana’s waiver also applies to other groups.)
Kentucky has a request pending that, like Iowa, would eliminate retroactive Medicaid eligibility except for pregnant women and children under 1, according to KFF.
Under federal law, officials can waive some Medicaid coverage rules to give states flexibility to experiment with different approaches to providing services. And retroactive eligibility waivers in Medicaid are hardly new. A few states like Tennessee have had them in place for years. Tennessee officials eliminated retroactive eligibility for all Medicaid beneficiaries in 1994 when the state significantly expanded coverage under TennCare, as Medicaid is known there. At the time, the state even allowed uninsured people to buy into the program who wouldn’t otherwise qualify based on income, said Bonnyman.
“There was no reason for anybody to be uninsured except undocumented immigrants,” said Bonnyman. “It didn’t seem to have the potential for harm.”
But state officials revamped that program after serious financial problems. Eligibility for TennCare has become more restrictive again.
Other states that waived retroactive coverage for at least some Medicaid groups include Delaware, Maryland, Massachusetts and Utah, according to the Kaiser Family Foundation.
Bonnyman said his group frequently works with Medicaid beneficiaries who have medical bills they can’t afford that accumulated during the months before they applied for Medicaid.
“If you’re a moderate- to low-income working family, one or two days in the hospital is enough to ruin you financially,” he said.
You can read the original article here.
Source:
Andrews M. (14 November 2017). "Some States Roll Back ‘Retroactive Medicaid,’ A Buffer For The Poor — And For Hospitals" [Web blog post]. Retrieved from address https://khn.org/news/some-states-roll-back-retroactive-medicaid-a-buffer-for-the-poor-and-for-hospitals/

Understanding your Letter 226-J
Letter 226-J is the initial letter issued to Applicable Large Employers (ALEs) to notify them that they may be liable for an Employer Shared Responsibility Payment (ESRP). The determination of whether an ALE may be liable for an ESRP and the amount of the proposed ESRP in Letter 226-J are based on information from Forms 1094-C and 1095-C filed by the ALE and the individual income tax returns filed by the ALE’s employees.
What you need to do
- Read your letter and attachments carefully. These documents explain the ESRP process and how the information received affects the computation.
- The letter fully explains the steps to take if you agree or disagree with the proposed ESRP computation.
- Complete the response form (Form 14764) indicating your agreement or disagreement with the letter.
- If you disagree with the proposed ESRP liability, you must provide a full explanation of your disagreement and/or indicate changes needed on Form 14765 (PTC Listing). Return all documents as instructed in the letter by the response date.
- If you agree with the proposed ESRP liability, follow the instructions to sign the response form and return with full payment in the envelope provided.
You may want to
- Review the information reported on Forms 1094-C and 1095-C for the applicable year to confirm that the information filed with the IRS was accurate because the IRS uses that information to compute the ESRP.
- Keep a copy of the letter and any documents you submit.
- Contact us using the information provided in the letter if you have any questions or need additional time to respond.
- Send us a Form 2848 (Power of Attorney and Declaration of Representative) to allow someone to contact us on your behalf. Note that the Form 2848 must state specifically the year and that it is for the Section 4980H Shared Responsibility Payment.
Answers to Common Questions
Why did I receive this letter?
The IRS used the information you provided on Forms 1094/5-C and determined that you are potentially liable for an ESRP.
Where did the IRS get the information used to compute the ESRP?
The IRS used form 1094/5-C filed by the ALE and the individual income tax returns of your full-time employees to identify if they were allowed a premium tax credit.
Is this letter a bill?
No, the letter is the initial proposal of the ESRP
What do I need to do?
Review the letter and attachments carefully and complete the response form by the date provided.
What do I do if the information is wrong or I disagree?
Follow the instructions in the letter to provide corrected information for consideration by the IRS. The IRS will reply with an acknowledgement letter informing you of their final determination.
Do I have appeal rights?
Yes, the acknowledgement letter that you receive will spell out all your rights, including your right to appeal.
General Information
For more info visit ACA information center for Applicable Large Employers
Here’s an excerpt from the 226J letter, and a link to the official sample.
Source:
IRS (9 November 2017). "Understanding your Letter 226-J" [Web blog post]. Retrieved from address https://www.irs.gov/individuals/understanding-your-letter-226-j